How vaccines may change the way we treat cancer
Author: Javier Bautista (@javibautista_)
Editor: Dan Jacobson
Artist: Talia Pittman
Taking 165,000 lives every year in the UK, cancer represents one of the leading causes of death. Now imagine the possibility of using a personalised vaccine that can be injected into your body and help fight cancer. This is a medical strategy that has emerged in the last decade and it is showing promising results, but how can they be effective?
Cancer is caused by genetic mutations in our body that lead to abnormal cell growth. Therapeutic cancer vaccines are a promising strategy to stimulate a specific immune response to fight the patient’s cancer. But before we start the war, we need to introduce the protagonist in our story who will differentiate the cancer cells from the rest of our body: the neoantigens. These are signature proteins present on the surface of tumours that play an important role in initiation, progression and spread. To our advantage, neoantigens can be synthesised to betray the tumour and reveal the secrets to our own immune system in order to develop specific immune responses.
This is because cancer vaccines are like ‘WANTED’ posters. They just show the people from the village what the bad guys looks like, so that when facing them, people can recognise them and recruit others to fight them. Similarly, the principle behind cancer vaccines is to increase the supply of neoantigens in our body that reveal how the cancer looks like. These can be recognised by antigen-presenting cells, which are immune cells that serve as mediators and can activate other immune cells, like killer T-cells, that can recognise and fight the tumour.
The first step involves obtaining a sample of the tumour and analysing its DNA and RNA sequences. Bioinformatics analysis use next-generation sequencing, which compares the healthy and tumour genomes to the reference genome. This helps identify the genetic mutations and the specific neoantigens associated with the patient’s tumour. This can also have a positive impact in patients with rare mutations, where unique neoantigens can be identified to generate a personalised immune response against the cancer. After this, three different vaccine strategies can be employed (Figure 1): 1) gene-based vaccines, including DNA and RNA vaccines, 2) protein-based vaccines and 3) cell-based vaccines.
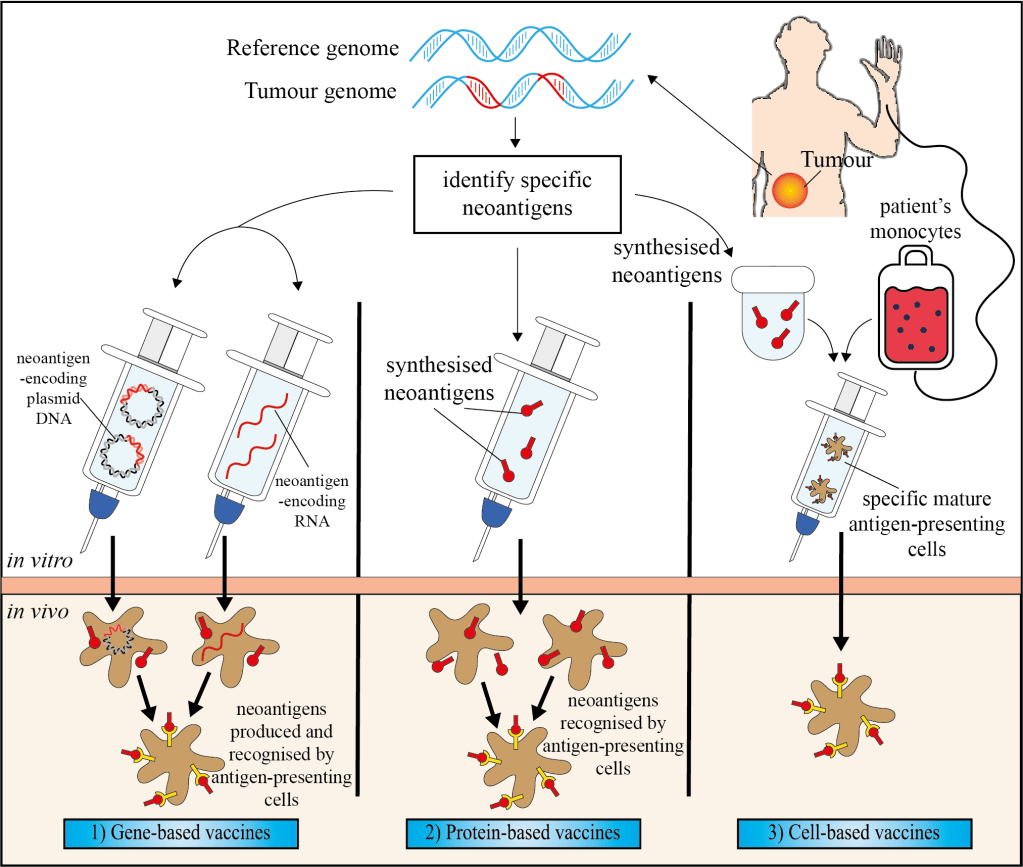
- Gene-based vaccines
Either a plasmid (extrachromosomal) DNA or an RNA strand are designed to deliver genes encoding neoantigens. When these are injected into the patient, the neoantigens are produced and recognised by antigen-presenting cells, which then elicit responses by the immune system against the tumour.
- Protein-based vaccines
The vaccines contain synthetic long proteins that contain the neoantigens. Once the vaccine is injected, the antigen-presenting cells will recognise the neoantigens, stimulating an immune response against the tumour.
- Cell-based vaccines
In contrast to the other strategies, this type of vaccine uses patient’s monocytes (immune white blood cells) which are exposed to synthesised neoantigens outside the patient’s body. After these monocytes become specific mature antigen-presenting cells, they are injected into the patient to trigger the immune response.
Several therapeutic cancer vaccines have already been designed, and so far, only two cancer vaccines have been approved by the Food and Drug Administration: Talimogene laherparepvec (T-VEC) to treat advanced melanoma skin cancer, and Bacillus Calmette-Guérin (BCG) to treat early-stage bladder cancer. However, the effect of these cancer vaccines may be reduced in patients with a weakened immune system due to age, sickness or the presence of large tumours, suggesting that vaccines might only be useful for fighting smaller tumours or early-stage cancers. In the future, the issues associated with non-efficient monotherapy may be approached by employing combinational therapy with radiotherapy or chemotherapy, which has been shown to have greater clinical benefits.
At this point, cancer vaccines may seem very appealing. However, although they have been reported to treat cancer, most of these vaccines are not easily accessible. In the UK, patients usually gain access to this therapy through ongoing clinical trials. Additionally, there are two social factors that may affect their future prevalence. On the one hand, even with the approval of these vaccines by The Medicines and Healthcare products Regulatory Agency in the UK, exorbitant prices may deem these treatments inaccessible for a wide range of the population. On the other hand, with the growth and evolution of the anti-vaxxer movement, some patients may be reluctant to choose this therapy. This could potentially extend to campaigns against the development of these vaccines, decreasing the funding to improve this novel therapy.
Although it may sound like science fiction to inject a vaccine to kill cancer cells, this molecular research is currently being developed. We still need to wait to see how successful this therapy could be, but hopefully, one day, we can successfully fight cancer with personalised vaccines and prevent the suffering of people with genetic mutations.
